The biggest drawback of IC management is that we do not know which treatment will treat which patient. Multiple treatment options are available like therapeutic hydrodistension, oral therapy, intravesical therapy which includes instillations and injections, neuromodulation and surgery. We try one treatment after other in quick succession and stop when patient improves.We believe that there is always some treatment available for all patients but there is no test to find out which treatment will benefit which patients.No center in the world including us can guarantee cure for this disease.
With our experience and devotion to IC/BPS we feel that we can definitely help all the patient. A correct diagnosis saves patients from unnecessary medications and procedures.9 out of 10 patients improve at our center. We have published our long term 20 yearsresults. We firmly believe there is no shortcut for treating IC/BPS. We follow a rigorous protocol for managing IC/BPS. We strictly follow this protocol as we consider it as bestoption for the patients. As etiopathology of IC/BPS is not known we believe that multimodal therapy gives best results in IC/BPS patients.
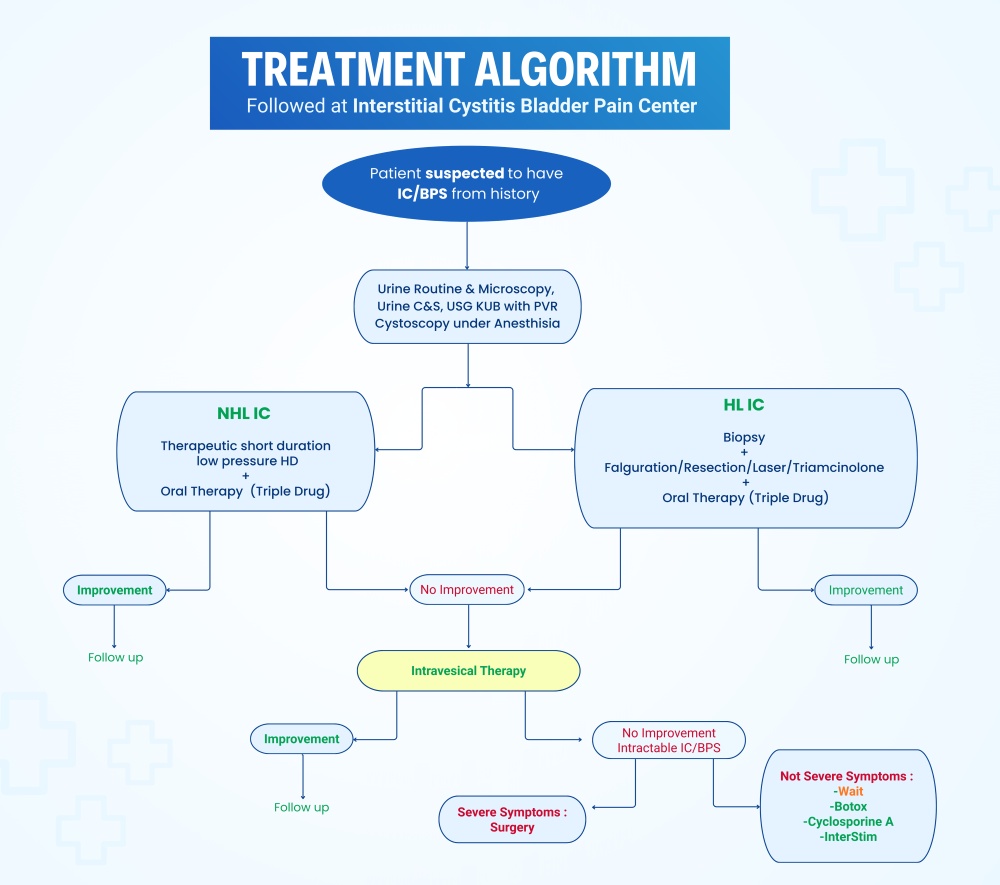
1. cystoscopy therapeutic hydrodistension with oral therapy
All the patients are subjected to diagnostic cystoscopy and therapeutic hydrodistension after their urine routine/urine culture, and sonography are normal. Cystoscopy is done under spinal anaesthesia and the bladder is distended under gravity till capacity. No attempt is done to overdistend the bladder.We prefer spinal anaesthesia as post cystoscopy recovery is comfortable after spinal anesthesiawhereas after general anaesthesia post procedure patients are very uncomfortable.Patients with normal bladder capacity are put on triple drug therapy including amitriptyline, hydroxyzine and gabapin or Pentosan for 3 months. It is important to note that the routine analgesics and antibiotics do not act on such patients and should not be prescribed alone. If hunners lesions are found on hydrodistension then coagulation of the lesions is done at the same time.
2. intravesical therapy
If the patient does not respond or there is flare-up during oral therapy, the patient is treated with intravesical cocktail rescue solution. The rescue solution is prepared by mixing an anaesthetic agent with steroid and heparin. The solution is usually kept in the bladder for 30 minutes and 6 treatments are given at intervals of 2 weeks. My favourite rescue solution consists of 40 ml sensorcaine 0.5%, 2cc dexamethasone and 25000 unit of heparin. 50% patients improve with this intravesical therapy.If the patient does not improve with one rescue solution then other intravesical therapies can be tried.
We also instil intravesical Tacrolimus in our patient especially with hunners lesion. This intravesical therapy has been developed by us in 2013 and we have used for the first time in the world in human beings. Till now we have used intravesical Tacrolimus in more than 100 patients with success in 50%.
3. surgery
Surgery is offered as a last resort and various procedures are available with varying success rates. Surgery is offered to those patients who have a miserable life and have failed all other therapies. On cystoscopy under spinal anaesthesia if patient has less than 150 ml maximal bladder capacity he is advised surgery to increase bladder capacity or to replace bladder.
At this center we have expertise of doing Clam patch cystoplasty and till now we have done surgery in 23 patients. 4 patients have died due to cause unrelated to surgery. 19 patients are surviving and all patients have improved. 16 patients are symptom free. The longest followup is of 13 years and the patient is symptom free. We offer surgery to all the patients who do not improve after adequate treatment and are suffering from severe disease.
We believe in taking time bound decision for surgery if patient is not improving. Our policy is not to linger with the treatment and let the patient suffer for a long time. For a patient with severe disease and not improving removal of bladder is also a good option. We offer a new bladder in these patients
Abbreviations
1. IC/BPS- Interstitial Cystitis/ Bladder Pain Syndrome, 2. HLIC- Hunners Lesion IC/BPS, 3. NHLIC- Non Hunners lesion IC/BPS 4. USG KUB- Ultrasonography of Kidney, Ureter and Bladder 5. PVR- Post Void Residue 6. HD- Hydrodistension
Abbreviations
1. IC/BPS- Interstitial Cystitis/ Bladder Pain Syndrome, 2. HLIC- Hunners Lesion IC/BPS, 3. NHLIC- Non Hunners lesion IC/BPS 4. USG KUB- Ultrasonography of Kidney, Ureter and Bladder 5. PVR- Post Void Residue 6. HD- Hydrodistension